Wednesday, April 8, 2026
How to Redesign Your PT Practice Around Patient Need


Match care intensity to patient profile instead of defaulting to a single protocol
When Ben Barron talks about the PT market, he sounds like someone watching a winning team leave points on the board.
The profession has won the clinical argument: demand is growing faster than the rest of healthcare, the country is short by at least 12,000 PTs, and every other provider in the MSK continuum is being told to send more patients to conservative care.
But most practices aren't capitalizing on that, and if they don't change, Ben says they're looking at a slow bleed: declining reimbursements, thinner margins, and eventually, a business that can't survive.
Key Takeaways:
- Established practices face different constraints than startups: existing payer contracts, staff expectations, and patient populations require change management, not greenfield design.
- The three leverage points (wait list management, payer contract hygiene, and care model design) are interdependent and must be addressed in sequence.
- PT practices have growth available through model redesign before spending another dollar on new patient acquisition.
When You Build for Scarcity, You’re Stuck With Scarcity
Ben has spent many years in the PT world. Part of his journey includes building and selling a multi-location physical therapy practice in New England. Through that process, he’s seen how the standard PT business model is designed and operating for a world where patients are scarce.
In the past, practices fought over a finite referral pool, and every payer contract, scheduling decision, and care protocol reflected that.
The care model defaulted to two-to-three visits per week for six-to-eight weeks at forty-minute intervals because that's how the Medicare eight-minute billing rule produced the least waste.
The business emulated the economic model, and the economic model was never designed to optimize health.
Today, the constraint has flipped. Physical therapy is the only service line the system is actively pushing patients toward. But practices with waitlists are rationing care on a first-come, first-served default instead of by design. Therapists are doing doctoral-level work and rep-counting work in the same hour.
KPIs like visit volume, eval volume, and other general productivity metrics incentivize raw numbers over reach. Payer contracts signed years ago are quietly compressing margin every year.
Practices are technically busy but structurally, they’re capped.
The Operating Logic Needs to Catch Up
If PT practices are running an abundance of patients through a scarcity-era model, Ben’s argument is that three things—wait list management, payer contract hygiene, and care model design—have to change, and they have to change in a specific sequence.
Operators who try to fix care models without addressing wait lists and contracts first will create change without meaningful gains. Operators who address all three in order will find compounding results.
This is not about going cash-pay or blowing up existing infrastructure. Ben explicitly frames this for established practices—operators who have existing contracts, existing staff expectations, and existing patient populations—and need a change management strategy.
The ABC of Operational Change Management
Ben built a sequenced framework that acknowledges the reality most practice owners face: you can't overhaul everything at once, but you can be deliberate about which changes create the scaffolding for others.
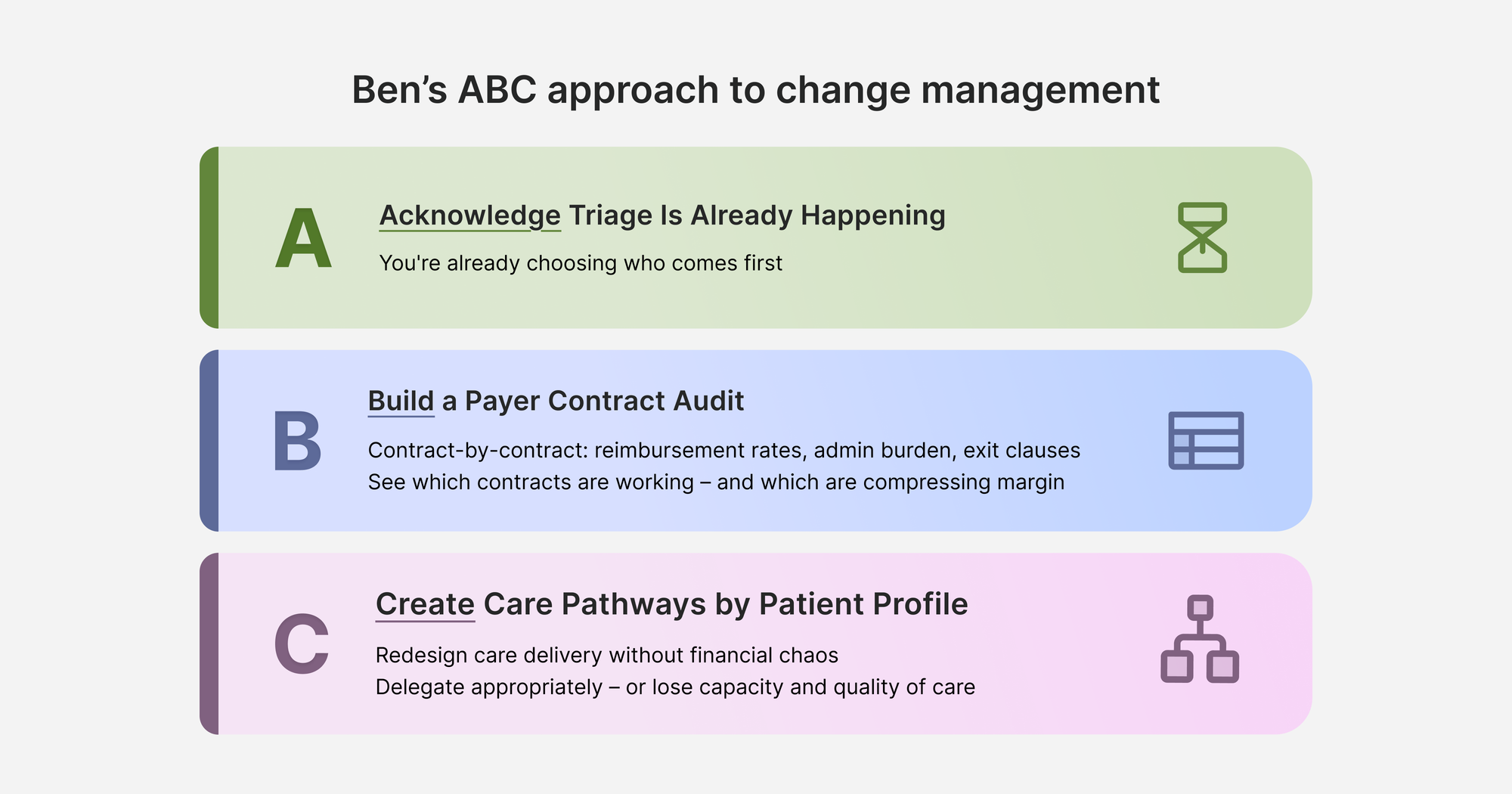
Acknowledge You're Already Making Triage Decisions
Every practice with a waitlist is already rationing physical therapy care. It might be happening by accident, but it’s happening.
The first step is acknowledging that and replacing accidental rationing with intentional triage. Today, the way most practices decide who comes through the door is based on the order in which people pick up the phone. That's a choice, even if it doesn't feel like one.
"You are rationing physical therapy care,” Ben explains, “but you are choosing to ration it based upon when someone calls you as opposed to something else."
Ben offers two concrete models as examples.
One is payer-mix-based prioritization: routing higher-reimbursing patients to the front of the line.
Another is acuity-based prioritization: all post surgical patients get seen within 24 hours, regardless of waitlist position.
Neither model is prescribed as the right answer, they’re just examples of other ways care might be prioritized. The point is that operators should be choosing deliberately based on what aligns with their values and clinical focus.
Once operators understand who is and isn't getting through the door (and why), they're ready to look at the financial architecture underneath that.
Build a Payer Contract Audit
Once a practice understands its triage logic, the next question is whether the financial relationships underneath that logic actually support the business they want to build.
Most practice owners can name their payers. Very few can rank them by profitability, describe exit terms, or project when each contract renews.
Ben's recommended starting point: build a contract-by-contract spreadsheet that captures reimbursement rates by CPT code, administrative burden, renewal dates, and exit clauses.
The APTA has contracting resources that help operators assess contracts in totality, not just per-code rates, but overhead implications and admin load.
The goal isn't to exit all payer contracts or act on the audit right away. The audit creates visibility into which ones are working, which are compressing margin, and which can eventually be renegotiated or exited as waitlist pressure gives the practice more negotiating power.
When you have 40 people on your waitlist, you don't have to say yes to a bad contract. The economics fundamentally change at that point.
With triage logic defined and contract clarity emerging, operators now have the scaffolding to redesign care models without destroying existing revenue.
Create Care Pathways Based on Patient Profile
Once payer contracts are mapped and triage logic is running, practices can begin redesigning care delivery without financial chaos. Different patient profiles need different care pathways.
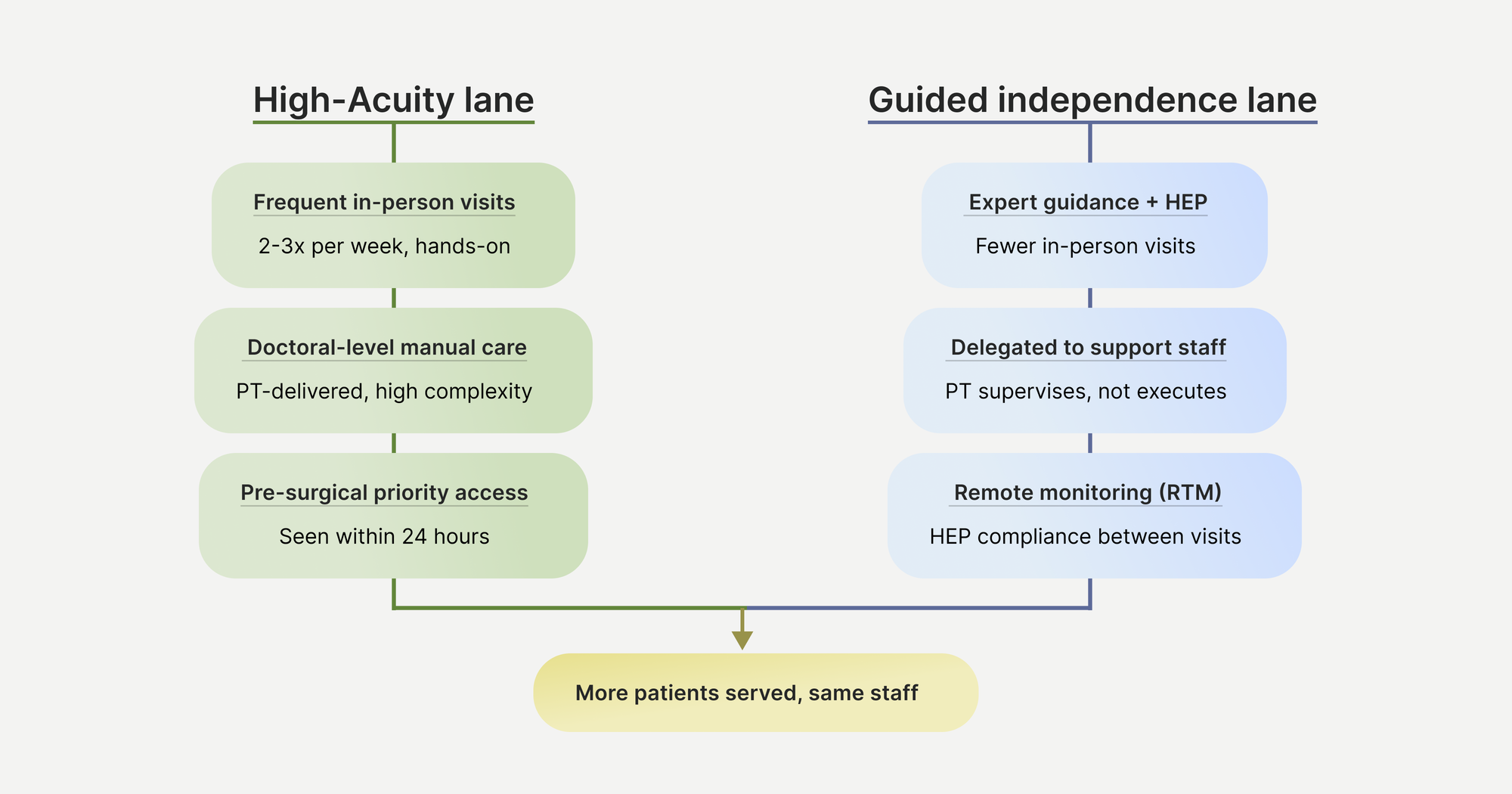
Ben sees these pathways through a swim lane analogy: one lane for high-acuity patients who genuinely need frequent in-person contact and significant manual treatment, and one lane for patients who need expert guidance, accountability, and monitoring but don't need someone counting their reps.
Depending on the practice's focus, other lanes could be added as well.
The lanes also mean delegation of work is better managed and accounted for.
"We are the only doctoring profession that says good care means being delivered by the person with the highest license," Ben observes. "Physical therapists have to count your repetitions, watch you do your thing, clean up the table. Imagine if you owned a best-in-class restaurant and the chef had to be the busser, the host, the server, and the chef. It's insane."
Practices that can't delegate appropriately are leaving both capacity and quality of care on the table.
Unlock Capacity Without New Hires
When practices stop measuring throughput as the primary KPI and start measuring lives reached plus outcomes achieved, capacity opens up. Swim-lane patients who need fewer in-person visits free up therapist time for higher-acuity cases. More new patients get in the door.
Plus, the practice's leverage in payer negotiations improves, and contract audits help them see where that leverage should be applied. Care can extend beyond clinic visits. Remote therapeutic monitoring codes allow practices to track home exercise compliance and communicate with patients between appointments, creating value without requiring more face-to-face time.
For established practices struggling with demand that exceeds supply, the solution is redesigning the operating logic to match the market you're actually in.
Frequently Asked Questions:
How can PT practices increase capacity without hiring more therapists?
PT practices can increase capacity by implementing a swim lane care model that matches treatment intensity to patient need. Patients who need expert guidance but not constant supervision can follow self-directed care pathways with fewer in-person visits, freeing up therapist time for high-acuity cases requiring frequent hands-on treatment.
This approach allows practices to serve more patients with existing staff by stopping the practice of having doctoral-level clinicians perform tasks like counting repetitions that don't require their expertise.
What is a payer contract audit and why do PT practices need one?
A payer contract audit is a contract-by-contract spreadsheet that captures reimbursement rates by CPT code, administrative burden, renewal dates, and exit clauses for every insurance relationship.
The audit creates visibility into which contracts compress margin and which can be renegotiated or exited as waitlist pressure gives the practice more leverage.
Why are PT practices rationing care by accident?
Most PT practices fill appointments based on who calls first, rather than clinical priority or business logic, and then builds a waitlist once those appointment slots are filled. This first-come, first-served approach is accidental rationing. Practices are already making decisions about who gets treatment, they're just doing it by chance instead of deliberately.
Intentional triage systems (like acuity-based prioritization where post surgical patients get seen within 24 hours, or payer-mix prioritization) allow practices to align patient access with their clinical values and financial sustainability.
What is the swim lane care model for physical therapy practices?
The swim lane care model creates different treatment pathways based on patient profiles rather than using a single protocol for everyone. One lane serves high-acuity patients who need frequent in-person contact and significant manual treatment, while another serves patients who need expert guidance and accountability but can follow more independent care plans.
Each lane has differentiated success metrics. This model allows practices to serve more patients while improving outcomes.